
Many of SILK Medical intended parents focus on embryo quality, surrogate matching, and legal paperwork. For them, delivery often feels like a distant detail. In reality though, the method of birth plays an important role in how a surrogacy program is structured.
Cesarean delivery is common in surrogate pregnancies. Sometimes it is medically required. In other cases it is planned in advance because of a prior uterine scar or obstetric history. It is best for intended parents to know in advance when a C-section is likely to happen, how previous surgeries affect surrogate eligibility, and how recovery works.
When Is a C-Section Required in Surrogacy?
A cesarean delivery may be required for several medical reasons. The most common include placenta previa, fetal distress, breech presentation, stalled labor, or a large baby. Twin pregnancies also increase the likelihood of surgical delivery.
In many surrogate pregnancies, the decision is made in advance rather than during an emergency. If the surrogate has a prior uterine scar, the obstetrician may recommend a planned repeat C-section. This approach reduces the risk of uterine rupture and allows the team to coordinate timing, hospital admission, and legal steps related to birth registration.
According to the World Health Organization, cesarean delivery rates have increased globally over the past decades, particularly in medically supervised settings. You can review current global data here:
Sexual and Reproductive Health and Research (SRH).
In surrogacy programs, planned delivery is often preferred because it provides predictability for everyone involved.
How Prior C-Sections Affect Surrogate Eligibility
A prior C-section does not automatically disqualify a surrogate candidate. Most clinics accept women with one or sometimes two previous cesarean deliveries, provided the uterus has healed properly and there were no major complications.
During screening, SILK Medical doctors evaluate the number of prior surgeries, the type of uterine incision used, and the integrity of the scar tissue. Ultrasound assessment of the uterine wall helps determine whether it is safe to proceed with another pregnancy.
After three or more cesarean surgeries, the risk profile increases significantly. The likelihood of complications such as placenta accreta or uterine rupture becomes higher, and many clinics decline those candidates for safety reasons.
This medical screening is done before contract signing, so intended parents are not exposed to unexpected risk later in the program. In fact, in SILK Medical programs, it’s up to intended parents to specify ahead of time whether a candidate with a prior C-section can be shortlisted for their program.
Why Repeat C-Sections Are Common in Surrogacy
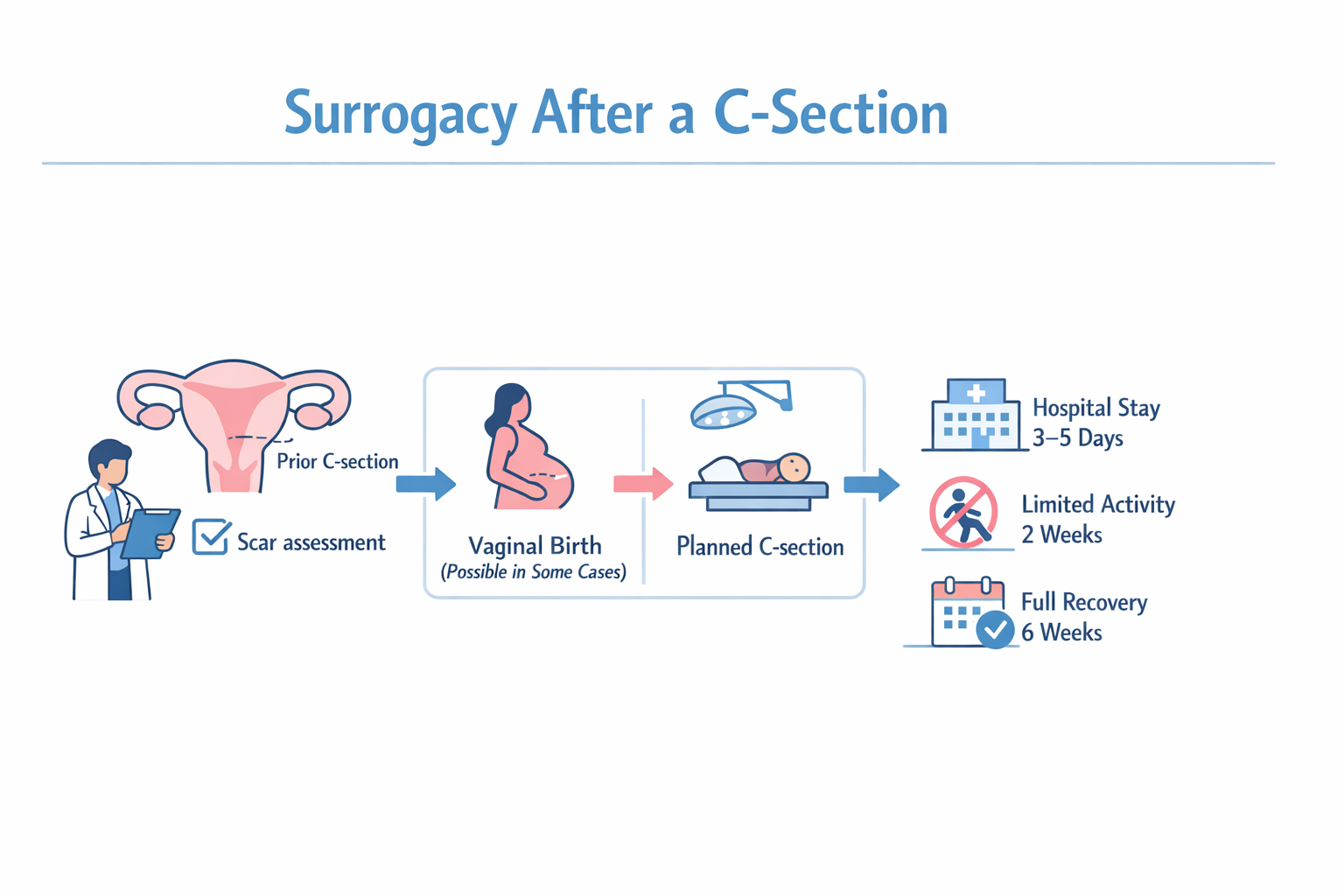
After one cesarean delivery, vaginal birth after cesarean, known as VBAC, may still be possible. However, many obstetricians recommend repeat C-section, especially if the surrogate has already had more than one surgical birth.
Repeat cesarean delivery is common in surrogacy because it lowers the risk of uterine rupture in women with prior scars and avoids prolonged labor that could stress the uterine wall. It also allows coordinated timing for intended parents who are traveling from abroad and reduces uncertainty around delivery logistics.
Planned surgery also makes it easier to prepare hospital documentation and legal paperwork in advance, which is particularly important for international intended parents.
Recovery Timeline After a C-Section
Cesarean delivery is major abdominal surgery. Recovery requires time and monitoring.
The surrogate typically stays in the hospital for three to five days. Physical activity is limited during the first two weeks, and gradual return to normal movement usually occurs over four to six weeks. Scar healing continues for several months.
Pain management, infection monitoring, and wound care are part of standard post-operative follow-up. Surrogates are monitored medically during this period, and compensation structures reflect the additional recovery time required compared to vaginal delivery.
The American College of Obstetricians and Gynecologists provides detailed guidance on cesarean recovery and indications: Cesarean Birth | ACOG.
How C-Section Affects Surrogacy Program Costs
Surgical delivery involves operating room use, a surgical team with anesthesia, longer hospitalization, and increased medical supervision.
In SILK Medical’s Classic and Successful programs, C-section delivery carries a 2,000 USD add-on, while in the Guaranteed program, C-section delivery is included with no additional charge
The difference reflects how each program is structured financially. In the Guaranteed model, surgical variability is absorbed into the overall package. In other programs, it is defined separately as a surgical expense.
What Intended Parents Should Focus On
A prior C-section does not make a surrogate unsafe by default. The key factors are careful screening, proper scar assessment, and experienced obstetric management.
Repeat cesarean delivery is common in surrogacy because it offers predictability and reduces certain medical risks. Recovery takes longer than vaginal birth, which is why programs account for it both medically and financially.
For SILK Medical’s intended parents, the main priority should be whether the surrogate has been medically evaluated according to clear criteria and whether delivery planning is coordinated in advance. When those steps are handled properly, cesarean delivery becomes a structured medical event rather than an unexpected complication.
