
Most explanations of surrogacy focus on two points. The embryo transfer, and the delivery. What happens in between is usually reduced to a vague “pregnancy monitoring” phase, even though this period takes up most of the timeline and carries its own structure, logistics, and decisions.
The stretch between week 12 and week 28 is treated at SILK Medical as a distinct stage of the program, with defined medical routines, living arrangements, and coordination between teams in different locations. It is also the phase where most of the day-to-day work happens, even if very little of it is visible from the outside.
What Changes After Week 12
By week 12, the pregnancy is considered clinically stable. The early risks associated with implantation and initial development are significantly lower, and the focus shifts from reproductive medicine to standard obstetric care.
At this point, there is no longer a need for intensive hormonal support or close post-transfer observation. The program moves into a routine rhythm built around scheduled checkups, ultrasound scans, and ongoing supervision.
This is also when the structure of the surrogacy program becomes more visible. The medical side becomes predictable, but coordination, logistics, and communication take on a larger role.
Where the Surrogate Lives During This Period
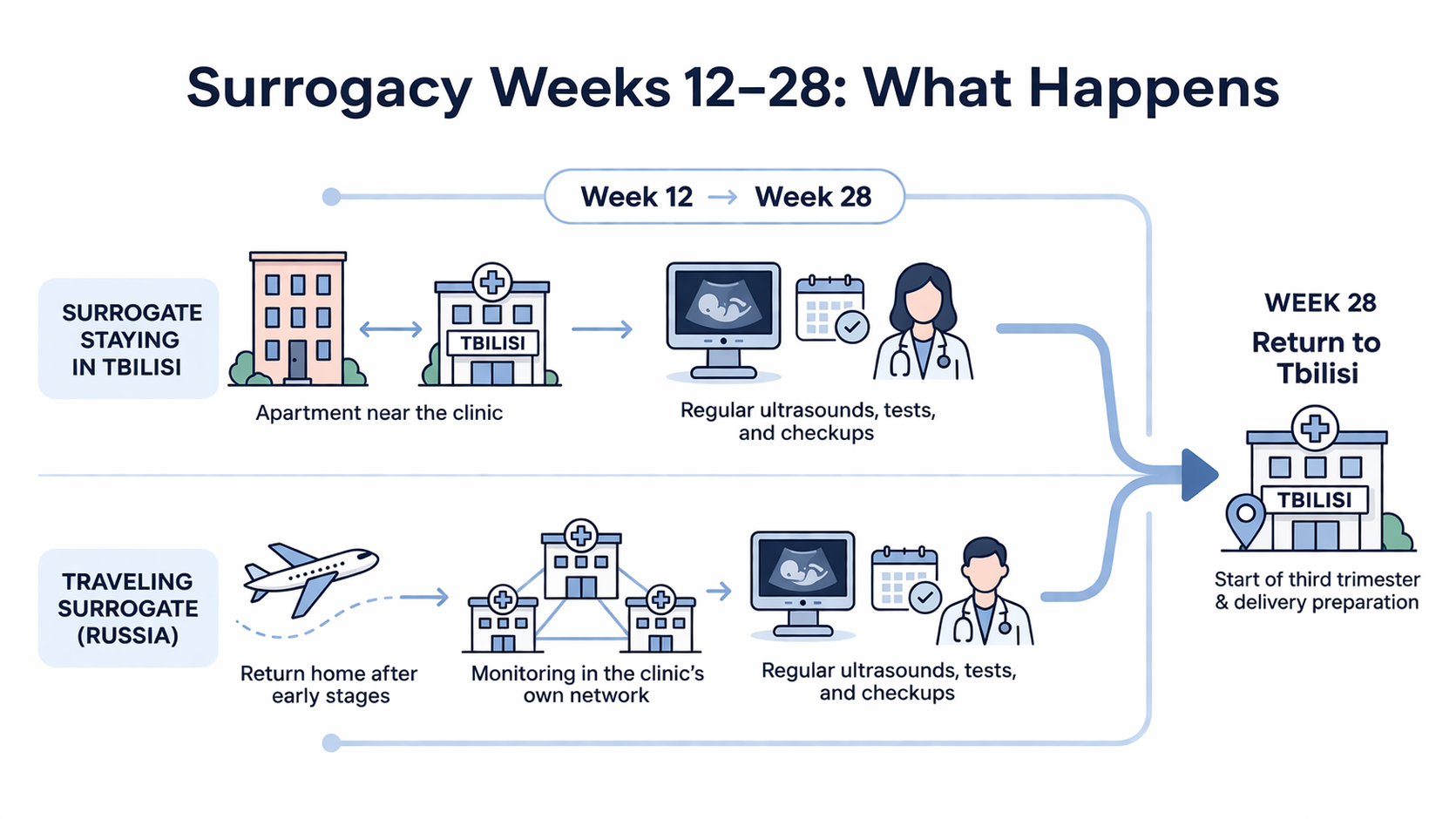
From week 12 onward, the surrogate’s location depends on the model chosen at the start of the program.
In cases where the surrogate stays in Georgia, accommodation is arranged in Tbilisi, typically in modern apartments located within walking distance of the clinic. This allows for regular in-person monitoring and quick access to doctors if needed. Daily life remains stable, with appointments scheduled in advance and coordinated by the clinic team.
For traveling surrogates, the setup is different. After the embryo transfer and early confirmation stages, they return to their home country, most commonly Russia. This is not handled through external partner clinics. Instead, monitoring continues within the clinic’s own network, which includes over 30 facilities across Russia. These locations operate under the same protocols, with local doctors and coordinators working in direct contact with the main team in Tbilisi.
This model allows the surrogate to remain in a familiar environment during the second trimester while still being under continuous medical supervision.
Medical Monitoring Between Week 12 and 28
During this period, monitoring follows a standard obstetric schedule. The surrogate attends regular ultrasound examinations, blood tests, and routine checkups to track fetal development and overall health.
Even when the surrogate is outside Georgia, the coordination remains centralized. Medical reports, scan results, and updates are shared with the main team, and any adjustments to care are communicated back through coordinators and supervising doctors.
The process is structured and consistent. There are no gaps in supervision, and no stage where the pregnancy is left unmanaged. This continuity is part of how the program maintains stability across different locations.
Communication With Intended Parents
Communication during this phase is steady and structured. Intended parents receive updates after key appointments, including ultrasound results and general progress reports.
Most of the interaction is handled through coordinators, who act as the main point of contact between the parents, the surrogate, and the medical team. This keeps communication clear and avoids confusion or conflicting information.
Direct communication with the surrogate can also be arranged depending on the situation, but it is usually guided to keep expectations and boundaries clear on both sides.
Monthly Compensation and Ongoing Support
After pregnancy confirmation, the surrogate begins receiving monthly compensation, which continues throughout the pregnancy. These payments are part of the agreed structure and cover daily living needs during this period
In addition to financial support, all medical care, transportation for appointments, and coordination are managed as part of the program. If the surrogate is based in Tbilisi, housing is provided. If she is in her home country, local supervision and logistics are handled through the clinic’s network.
This stage is generally intended for maintaining consistency over several months.
Why Week 28 Matters
Week 28 marks the transition into the third trimester. At this point, all surrogates return to Tbilisi, regardless of where they were based during the earlier stage.
From here, monitoring becomes more frequent, and preparation for delivery begins. The surrogate is placed under direct supervision of the local medical team, with access to the clinic and partner maternity hospitals.
This return is planned in advance and is a standard part of the program structure. It aligns medical oversight, logistics, and legal preparation in one place ahead of delivery.
What Can Come Up During This Period
The second trimester is generally stable, but it still requires consistent monitoring. Routine issues can appear, and when they do, they are addressed through scheduled care rather than emergency intervention.
Because the process is structured and supervised throughout, any changes in the pregnancy are detected early. The focus during this phase is placed on maintaining steady conditions through regular follow-up and coordination.
The Longest Part of the Program, and the Most Structured One
Between week 12 and week 28, there are no major milestones like transfer or delivery, but this is where most of the program actually unfolds. Medical care follows a steady schedule, living arrangements are already in place, and communication runs through a fixed structure that stays consistent for months.
This is also the stage where differences between clinics become easier to see. The medical side is fairly standard everywhere, but the way monitoring is organized across countries, how surrogates are supported in daily life, and how information flows between all parties can vary a lot.
SILK Medical builds this period around continuity, with the same team coordinating care whether the surrogate is in Tbilisi or within the clinic’s network abroad, and then bringing everything back under one roof from week 28 onward.
