
PGT-A and PGT-M tend to come up early in IVF discussions, often before there is a clear sense of what each test actually does. Many patients hear both terms during the planning stage, usually around the time embryo creation is being considered, and assume they are variations of the same procedure.
In practice, they serve different purposes. One focuses on the number of chromosomes in an embryo, while the other looks for specific inherited genetic conditions. Clinics like SILK Medical offer these tests as part of certain IVF programs, so the question is not only what they are, but whether they are relevant in a given case.
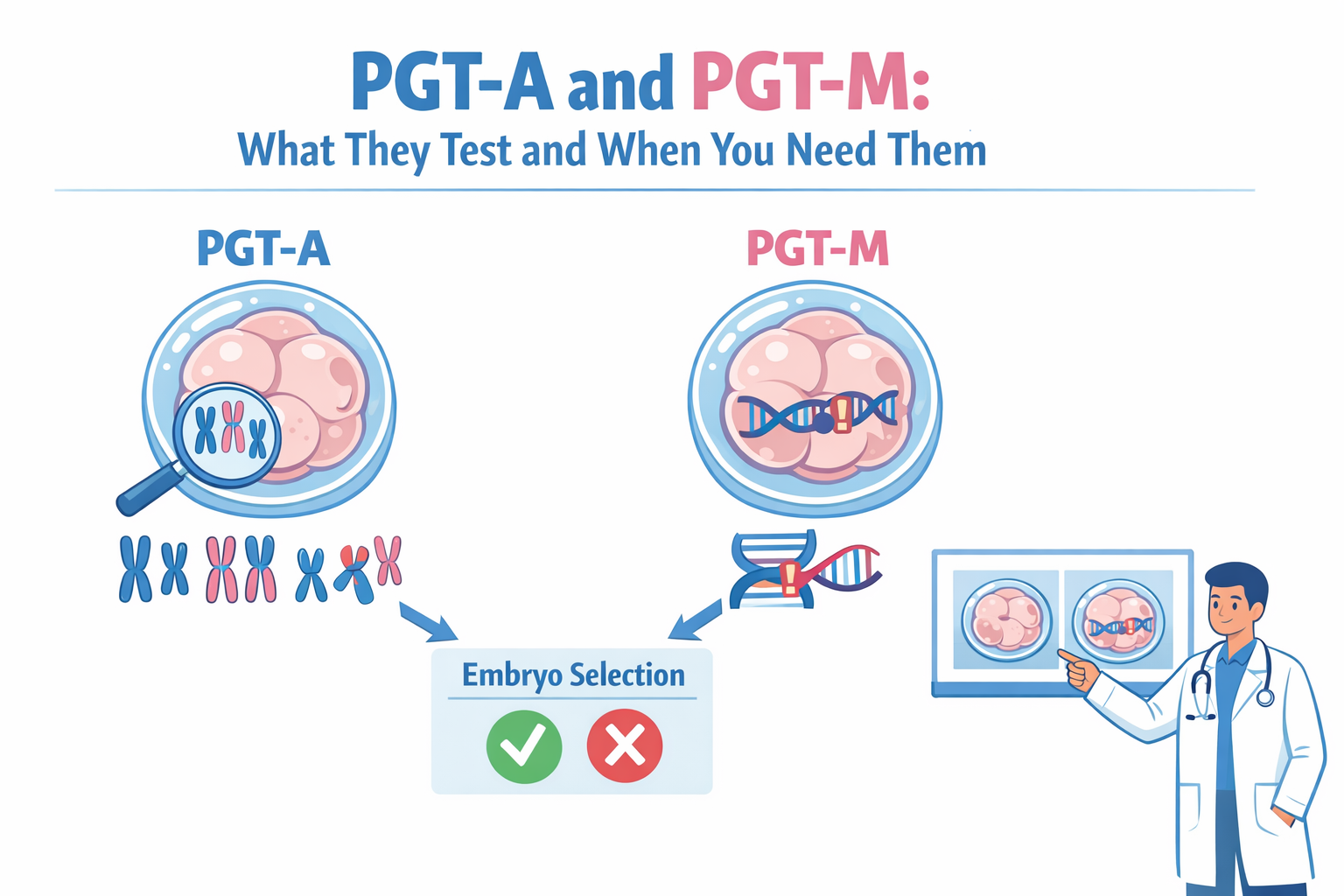
What PGT-A Actually Tests
PGT-A looks at the number of chromosomes in an embryo. A healthy embryo is expected to have 46 chromosomes, arranged in 23 pairs. When there is an extra or missing chromosome, the embryo is classified as aneuploid.
This type of imbalance is one of the most common reasons embryos fail to implant or result in early miscarriage. Conditions such as Down syndrome are linked to these chromosomal differences.
The test is performed on a small sample of cells taken from the embryo at the blastocyst stage, usually on day five or six. The embryo is then frozen while the sample is analyzed. The result helps identify which embryos have a normal chromosomal structure and are more suitable for transfer.
Keep in mind that PGT-A does not change the embryo. It only provides information that helps with selection.
What PGT-M Is Designed For
PGT-M focuses on specific genetic conditions that run in families. These are single-gene disorders, such as cystic fibrosis, spinal muscular atrophy, or thalassemia.
Unlike PGT-A, this test is only used when there is a known genetic risk. One or both partners must carry a mutation that could be passed on to the child. Before the IVF cycle begins, the lab develops a custom testing setup based on the exact mutation involved.
Once embryos are created, they are tested to determine which ones do not carry the condition. Only embryos without the targeted mutation are considered for transfer.
This type of testing is more targeted and requires additional preparation time compared to PGT-A.
PGT-A vs PGT-M: The Core Difference
PGT-A checks whether the total number of chromosomes is correct.
PGT-M checks whether a specific inherited disease is present.
An embryo can have the correct number of chromosomes and still carry a genetic condition, or it can be free of a specific mutation but have chromosomal abnormalities. In some cases, both tests are used together.
When PGT-A Is Typically Recommended
PGT-A is often considered in situations where the risk of chromosomal abnormalities is higher or where previous IVF attempts have not led to a successful pregnancy.
This includes women over 35, cases with repeated implantation failure, or a history of miscarriage. It is also commonly used when embryos are being prepared for surrogacy, where each transfer involves additional time and coordination.
Most IVF programs at SILK Medical include PGT-A for a set number of embryos as part of the overall package, with additional embryos tested separately if needed.
When PGT-M Becomes Necessary
PGT-M is used when there is a confirmed genetic condition that could be passed to the child. This may be known from family history, previous genetic testing, or the birth of an affected child.
In these cases, the goal is very specific. The testing identifies embryos that do not carry the condition, so that only those embryos are used for transfer.
Without this step, there is a significant risk of passing the condition to the child.
How Genetic Testing Fits Into the IVF Timeline
After fertilization, embryos are cultured in the SILK Medical embryological lab for several days. Around day five or six, when they reach the blastocyst stage, a small number of cells are taken for testing in a procedure called biopsy.
The embryos are then frozen. The biopsy samples are sent to a genetic lab, and results are usually available in about three weeks.
Once the results are ready, a frozen embryo transfer can be planned using an embryo that meets the desired criteria
Accuracy and Limits
Both PGT-A and PGT-M are highly accurate, but they do not cover every possible issue. PGT-A focuses on chromosome number and does not detect all genetic conditions. PGT-M targets a specific mutation and does not evaluate the overall chromosome structure unless combined with PGT-A.
There are also extremely rare cases where the sampled cells do not fully represent the entire embryo. Because of this, testing improves selection but does not remove all uncertainty.
Cost and How Testing Is Structured
In many clinics, including SILK Medical, genetic testing is priced per embryo, which can significantly increase the total cost of IVF.
Some programs include PGT-A for a limited number of embryos within the base price, while additional embryos are tested at a fixed per-embryo rate. This structure makes the total cost more predictable at the planning stage.
Why This Matters in Surrogacy Programs
When embryos are created for surrogacy, each transfer involves more coordination, time, and cost compared to a standard IVF cycle.
Using embryos that have already been tested for chromosomal normality can reduce the number of failed transfers. This is why PGT-A is commonly used in SILK Medical surrogacy programs, especially when working with donor eggs or when previous attempts have not been successful.
Many structured surrogacy programs include genetic testing as part of the embryo creation stage, particularly when multiple transfer attempts are planned
Choosing the Right Approach
PGT-A and PGT-M serve different roles, and the choice depends on the medical background of the patients and the goal of the IVF cycle. A consultation with SILK Medical reproductologist, and in some cases a geneticist is advised.
In some cases, no genetic testing is needed. In others, it becomes a central part of the process, especially when there is a known genetic risk or when previous outcomes make embryo selection more important.
